Understanding Risk in Healthcare for Consumers
Understanding Risk in Healthcare for Consumers
Jump to: Describing risk | Examples
Understanding Risk and Benefit
“Understanding health risks is key to making your own health care decisions. It gives you perspective on potential harms and benefits, so you can make smart choices based on facts and not fears.”[1]
When people talk about risk in health care, they are usually talking about the chance of a negative outcome (something bad) happening. This can be:
- an unpleasant or dangerous side effect of medication or treatment – such as a rash, headache or upset stomach
- your health getting worse – for example the treatment not working, or making you sicker
- getting a new health problem – like high blood pressure or diabetes
- a life-threatening incident – such as an interaction between two medicines that could kill you.
In health care, people also talk about the chance of a benefit (a good outcome) happening, for example getting better or living longer.
You may have to decide:
Is the chance of something bad happening more likely, or more important to you, than the possibility that something good will happen?
For example, you might have to decide if taking medicine every day to reduce the chance that you could have a stroke or heart attack in the future is worth the possible side effects of taking the medication?
The factsheet Making Sense of Your Health Risks from the National Institutes of Health can help you start to think about health risks.
Information to help you decide about risks and benefits
When making decisions about risks and benefits you need information about:
- How likely is it that something bad will happen to someone like you (your age, gender, with your medical conditions and ethnic background)?
- How bad that thing is and how much of an impact will it have on you? Everyone has different ideas about what is okay for them or their family.
- How likely is it that something good will happen to someone like you?
You can ask your doctor or other health professionals to talk to you, or give you information, to help you understand the answers to these questions.
This information can help you decide what is more important to you – the possible risk or risks, or the possible benefit. You might be willing to take a chance that the bad thing will happen if it means you might get the possible benefit. For example, you might decide that it is okay to risk feeling tired from a new medication if it means that you have a lower risk of a stroke in the future.
Your health provider can tell you about the possible outcomes (both good and bad), but they can’t give you definite and guaranteed outcomes. For example, your doctor can tell you that taking a medication means that you are less likely to have a stroke, not that it means you definitely won’t have a stroke.
Describing risk
Sometimes people use words to describe risk, and sometime they use numbers.
“Rare” and “common” are examples of words that describe risk. If your doctor uses words, make sure you understand what they mean. What a doctor means by “rare” or “common” may not be the same as what you think the term means.
There are different ways to use numbers to describe risk. Doctors may use a percentage to explain how common or uncommon an outcome is. A percentage means “out of 100” – a risk that affects 5% of patients, means 5 in every 100 people.
Sometimes, an outcome can affect fewer than 1 person in 100. You might find it easier to understand if your doctor talks about 1,000 people instead of using a percentage. It is easier to image 3 people out of 1,000 than 0.3 of a person. You can ask your doctor to tell you how many people out of 1,000 would have a negative outcome. Some people find it useful to imagine 1,000 people as all the people in your suburb, and 100 people as all the people in your street.
Ask your doctor to describe the risk in a way that works for you. You can also read more about how health professionals describe risk in this article.
Absolute vs Relative Risk
To understand the potential risks or benefits of a medical treatment or behaviour change, it helps to focus on “absolute risk”.
- Absolute risk is the chance of something happening, for example a health problem.
- Relative risk compares the absolute risk for one group of people to the absolute risk for another group of people.
Here is an example of the difference between absolute risk and relative risk.
- Absolute Risk Reduction: If you have this test every two years it will reduce your chance of dying from this cancer in the next 10 years from around 3 in 1000 to around 2 in 1000.
- Relative Risk Reduction: If you have this test every 2 years, it will reduce your chance of dying from this cancer by around one-third (or 30%) over the next 10 years. This compares the risk of the people who have the test with the risk of the people who don’t have the test.
The first number tells you what your actual risk is now (3 in 1000), and how it will change if you do the test (2 in 1000). The other number is also accurate, but it doesn’t help you understand what your risk actually is, or help you to decide if having the test every two years is worth it. This image from EUFIC can help you see the difference between absolute and relative risk.
Talking about absolute risk helps you understand the risks and benefits that apply to you, and make informed choices. You can ask your doctor to explain the absolute risk of different outcomes for you and your individual details.
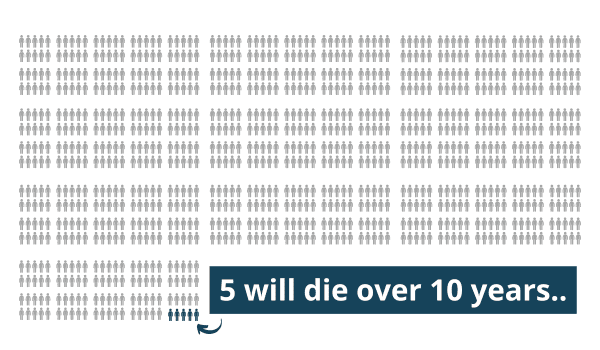
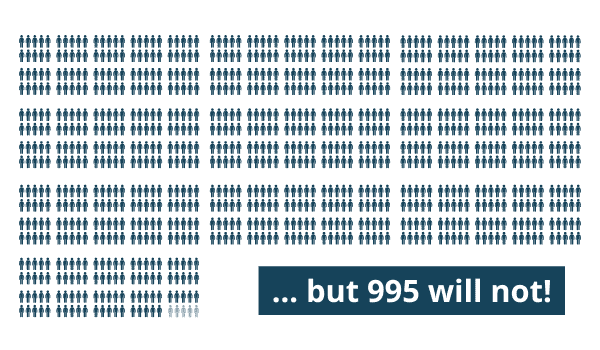
Re-frame the risk
To get the full picture, it can be helpful to reframe the risk. For example, if 5 out of 1,000 people will die over 10 years, it is also true that 995 out of 1,000 will not die. Ultimately, you want to know how likely it is that you will be one of the 5 out of 1,000 or one of the 995, and what you can do to improve the chance that you will be one of the 995.
It can help to use images when reframing the risk in your mind. Below is a picture showing those 1,000 people. Slide the bar to interact:
References:
[1] Elwood, William, cited in Understanding Health Risks – Improve Your Chances for Good Health at https://newsinhealth.nih.gov/2016/10/understanding-health-risks
Last Updated on 25 January, 2024.